Switch of breast tumors to HER2-low in recurrence may provide greater therapeutic options
The first study of its kind exploring how breast cancers change from the primary to the recurrent tumour has revealed that nearly 30% of breast cancer patients convert from, or to, human epidermal growth factor receptor (HER)2-low status. Specifically, the study found that 14% of triple-negative breast cancers with HER2-negative expression (also referred to as HER2-0) in the primary tumour converted to HER2-low expression in the recurrent tumour possibly offering an option to such hard-to-treat tumours.
Traditionally, breast cancers are categorised as: hormone receptor positive (HR+)/HER 2-negative, (also known as luminal-like), HER2-positive, or triple negative (negative for oestrogen receptors, progesterone receptors, and excess HER2 protein). HER2-low refers to HER2-negative tumours with low HER2 biomarker expression. About half of breast cancers classified as HER2-negative show low HER2 expression.
Presenting the findings at this year's ESMO Breast Cancer Virtual Congress is Dr Federica Miglietta, School of Oncology, University of Padua, Italy. (1) "The results provide a whole new insight on how HER2-low tumours might evolve as a subgroup, possibly challenging the current dichotomy between HER2-positive and HER2-negative breast cancer," she said. "Our findings stress the importance of re-testing HER2 expression on tumour relapse since it might provide the option of new therapeutic opportunities, currently in a trial, and hopefully in the near future, in the clinic." Several clinical trials are ongoing in HER2-low breast cancer.
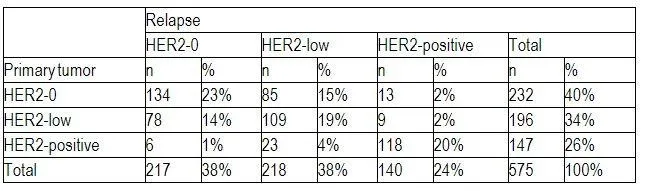
In total, 29% of recurrent breast cancer biopsies showed conversion either from, or to, HER2-low expression. In primary tumours and relapse tumours, HER2-low expression was seen in 34% and 38% of tumours, respectively. A total of 15% HER2-negative tumours switched to HER2-low tumours, and 14% HER2-low switched to HER2-negative.
The study also confirmed that HER2-low expression was more frequent in HR+/HER2-negative tumours compared to triple negative tumours (47% vs 36% on primary tumour samples, 54% vs 36% on relapse samples). Plus, the switch from HER2-negative to HER2-low in primary to recurrent tumours was 21% vs 14% in luminal-like and triple negative, respectively.
Commenting on the findings, Professor Aleix Prat, Head Medical Oncology, at the Hospital Clinic of Barcelona, Spain said: "These changes on HER2-low levels are substantial. There could be a biological rationale for this, or a technical one, given that there is currently no standardisation of how to determine levels of the HER2 biomarker in metastatic biopsies, which could be biopsied from skin, liver or bone and give different results."
"We need to work out how the HER2 status determines response to therapies - is it the HER2 status in the primary tumour, or in the metastatic biopsy that is important? Maybe some patients have HER2-low expression in metastatic tumours and now respond when they didn't previously, and this might change again over time and further relapses."
"This all speaks to a much greater need to biopsy metastatic tumours. Importantly, we need to determine who will benefit from treatments for HER2-low, because patients will be asking about this in the clinic soon if trial results are positive," said Prat.
INFORMATION:
Notes to Editors
Please make sure to use the official name of the meeting in your reports: ESMO Breast Cancer Virtual Congress 2021
Official Congress Hashtag: #ESMOBreast21
Disclaimer
This press release contains information provided by the author of the highlighted abstract and reflects the content of this abstract. It does not necessarily reflect the views or opinions of the ESMO who cannot be held responsible for the accuracy of the data. Commentators quoted in the press release are required to comply with the ESMO Declaration of Interests policy and the ESMO Code of Conduct.
References
1 https://www.esmo.org/meetings/esmo-breast-2021-virtual
2 Abstract 4MO_PR 'HER2-low breast cancer: evolution from primary breast cancer to relapse.' will be presented by Federica Miglietta during the Mini Oral Session 2 on Saturday, 8 May, 12:45-14:00 (CEST). Annals of Oncology, Volume 32, Supplement 2, May 2021
About the European Society for Medical Oncology (ESMO)
ESMO is the leading professional organisation for medical oncology. With more than 25,000 members representing oncology professionals from over 160 countries worldwide, ESMO is the society of reference for oncology education and information. ESMO is committed to offer the best care to people with cancer, through fostering integrated cancer care, supporting oncologists in their professional development, and advocating for sustainable cancer care worldwide. http://www.esmo.org
4MO_PR - HER2-low breast cancer: evolution from primary breast cancer to relapse.??
F. Miglietta1, G. Griguolo1, M. Bottosso1, T. Giarratano2, M. Lo Mele3, M. Fassan4, M. Cacciatore5, E. Genovesi1, D. De Bartolo4, G. Vernaci2, P.F. Conte1, V. Guarneri1, M.V. Dieci1
1Department of Surgery, Oncology and Gastroenterology (DISCOG), University of Padova, Padova, Italy,2Dipartimento di Oncologia 2, IOV - Istituto Oncologico Veneto IRCCS, Padova, Italy,3Surgical Pathology Unit, University Hospital of Padova, Padova, Italy,4Department of Medicine (DIMED), Surgical Pathology & Cytopathology Unit, University of Padova, Padova, Italy,5Department of Pathology and Molecular Genetics, Treviso General Hospital, Treviso, Italy
Background: About a half of breast cancers traditionally classified as HER2-negative show a low HER2 expression (IHC 1+ or IHC 2+ and ISH negative) that can be targeted by new antibody-drug conjugates. There is no data on the evolution of HER2-low status from primary tumor to relapse.
Methods: Patients with matched primary and relapse breast cancer samples from two Institutions (IOV-IRCCS Padova and Treviso Hospital) were included. HER2 was evaluated according to ASCO/CAP recommendations in place at the time of diagnosis. Cases diagnosed between 2007 and 2013 were reviewed by IHC to comply with the cutoff of >10% cells staining for HER2 positivity. Moreover, 100 random samples were reviewed by a blinded pathologist: agreement with the original report was 80%. HER2-neg cases were sub-classified as HER2-low (IHC 1+, or IHC 2+ and ISH not amplified), or HER2-0 (IHC 0).
Results: 575 patients were included. Primary?tumor?phenotype was: 59% luminal-like (HR+/HER2-neg), 25% HER2-pos, 16% triple negative. The proportion of HER2-low cases was 34% on the primary tumor and 38% on the relapse samples. Among HER2-neg cases, HER2-low status was more frequent in Luminal-like vs triple negative tumors (47% vs 41% on primary tumor samples, p=0.268;?54% vs 40% on relapse samples, p=0.006). The overall rate of HER2 discordance was 38% (Table 1), mostly represented by HER2-0 switching to HER2-low (15%) and HER2-low switching to HER2-0 (14%). A minority (9%) of cases lost or acquired HER2-positivity. Among patients with a primary HER2-neg?tumor, the rate of HER2 discordance was higher in luminal-like vs triple negative cases (45% vs 35% p=0.080). This difference was mostly driven by cases switching from HER2-0 to HER2-low: 40% of luminal-like/HER2-0 vs 24% of triple negative/HER2-0 patients (p=0.088).
Conclusions: HER2-low expression is highly unstable during disease evolution. Relapse biopsy in case of a primary HER2-0 tumor may open new opportunities for treatment in a relevant proportion of patients.
Legal entity responsible for the study: The authors
Funding: Has not received any funding
Disclosure: M.Fassan: Advisory/Consultancy, Research grant/Funding (institution), outside the submitted work: Astellas Pharma; Advisory/Consultancy, outside the submitted work:Diaceutics; Advisory/Consultancy, outside the submitted work:Tesaro; Research grant/Funding (institution), outside the submitted work: QED Therapeutics. P.F. Conte: Research grant/Funding (institution), outside the submitted work: Merck; Honoraria (self), Research grant/Funding (institution), outside the submitted work: Roche; Honoraria (self), outside the submitted work: Novartis; Honoraria (self), outside the submitted work: Lilly. V. Guarneri: Honoraria (self), Research grant/Funding (institution), outside the submitted work: Roche; Honoraria (self), outside the submitted work: Novartis; Honoraria (self), outside the submitted work: Eli Lilly. M.V. Dieci: Honoraria (self), outside the submitted work: Genomic Health; Honoraria (self), outside the submitted work: Eli Lilly; Honoraria (self), outside the submitted work: Celgene. All other authors have declared no conflicts of interest.