Study estimates two-thirds of COVID-19 hospitalizations due to four conditions
The study, published today in the Journal of the American Heart Association (JAHA) and led by researchers at the Gerald J. and Dorothy R. Friedman School of Nutrition Science and Policy at Tufts University, used a mathematical simulation to estimate the number and proportion of national COVID-19 hospitalizations that could have been prevented if Americans did not suffer from four major cardiometabolic conditions. Each condition has been strongly linked in other studies to increased risk of poor outcomes with COVID-19 infection.
"While newly authorized COVID-19 vaccines will eventually reduce infections, we have a long way to go to get to that point. Our findings call for interventions to determine whether improving cardiometabolic health will reduce hospitalizations, morbidity, and health care strains from COVID-19," said Dariush Mozaffarian, lead author and dean of the Friedman School. "We know that changes in diet quality alone, even without weight loss, rapidly improve metabolic health within just six to eight weeks. It's crucial to test such lifestyle approaches for reducing severe COVID-19 infections, both for this pandemic and future pandemics likely to come."
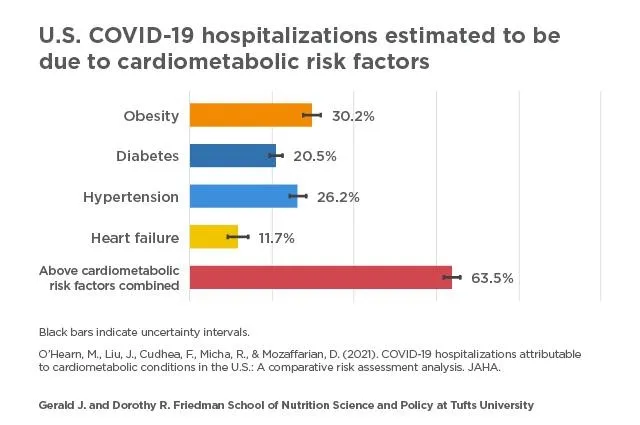
The researchers estimated that, among the 906,849 total COVID-19 hospitalizations that had occurred in U.S. adults as of November 18, 2020: 30% (274,322) were attributable to obesity; 26% (237,738) were attributable to hypertension; 21% (185,678) were attributable to diabetes; and 12% (106,139) were attributable to heart failure. In epidemiological terms, the attributable proportion represents the percentage of COVID-19 hospitalizations that could have been prevented in the absence of the four conditions. In other words, the study found the individuals might still have been infected but may not have had a severe enough clinical course to require hospitalization. When numbers for the four conditions were combined, the model suggests 64% (575,419) of COVID-19 hospitalizations might have been prevented. A 10% reduction in national prevalence of each condition, when combined, could prevent about 11% of all COVID-19 hospitalizations, according to the model.
The four conditions were chosen based on other published research from around the world showing each is an independent predictor of severe outcomes, including hospitalization, among people infected with COVID-19. The specific risk estimates for each condition were from a published multivariable model involving more than 5,000 COVID-19 patients diagnosed in New York City earlier in the pandemic. The researchers used other national data to model the number of COVID-19 hospitalizations nationally; the distributions of these hospitalizations by age, sex, and race; and the estimated distribution of the underlying comorbidities among adults infected with COVID-19. They then estimated the proportions and numbers of COVID-19 cases that became severe enough to require hospitalization owing to the presence of one or more of the conditions.
"Medical providers should educate patients who may be at risk for severe COVID-19 and consider promoting preventive lifestyle measures, such as improved dietary quality and physical activity, to improve overall cardiometabolic health. It's also important for providers to be aware of the health disparities people with these conditions often face," said first author Meghan O'Hearn, a doctoral candidate at the Friedman School.
The model estimated that age and race/ethnicity resulted in disparities in COVID-19 hospitalizations due to the four conditions. For example, about 8% of COVID-19 hospitalizations among adults under 50 years old were estimated to be due to diabetes, compared to about 29% of COVID-19 hospitalizations among those age 65 and older. In contrast, obesity had an equally detrimental impact on COVID-19 hospitalizations across age groups.
At any age, COVID-19 hospitalizations attributable to all four conditions were higher in Black adults than in white adults and generally higher for diabetes and obesity in Hispanic adults than in white adults. For example, among adults age 65 and older, diabetes was estimated to cause about 25% of COVID-19 hospitalizations among white adults, versus about 32% among Black adults, and about 34% among Hispanic adults.
When the four conditions were considered combined, the proportion of attributable hospitalizations was highest in Black adults of all ages, followed by Hispanics. For example, among young adults 18-49 years old, the four conditions jointly were estimated to cause about 39% of COVID-19 hospitalizations among white adults, versus 50% among Black adults.
"National data show that Black and Hispanic Americans are suffering the worst outcomes from COVID-19. Our findings lend support to the need for prioritizing vaccine distribution, good nutrition, and other preventive measures to people with cardiometabolic conditions, particularly among groups most affected by health disparities," Mozaffarian said. "Policies aimed at reducing the prevalence of these four cardiometabolic conditions among Black and Hispanic Americans must be part of any state or national policy discussion aimed at reducing health disparities from COVID-19."
INFORMATION:
Data
The model used existing data from several sources. Hospitalizations by age, sex, race and ethnicity came from the CDC's COVID-NET system, which tracks COVID-19 hospitalizations in 14 participating states. Data on national COVID-19 hospitalizations came from The COVID Tracking Project, a volunteer organization that collects data from all 50 states on the COVID-19 outbreak in the U.S. These two datasets were combined to estimate COVID-19 hospitalizations at the national level by population sub-groups. The data on the national distribution of the four conditions came from the most recent National Health and Nutrition Examination Survey (NHANES), a nationally representative study in which participants undergo medical examinations and laboratory tests. Data on the association between COVID-19 hospitalizations and each of the four conditions came from a study on factors associated with hospital admission among people with COVID-19 in New York City.
Limitations
The authors note that association does not equal causation, and the modeling approach does not prove reductions in the four conditions will reduce COVID-19 hospitalizations. Assumptions were based on limited available data on the cardiometabolic condition distribution among COVID-19 infected U.S. adults, the demographic breakdown of COVID-19 hospitalizations nationally, and the strongest evidence to date on links between cardiometabolic conditions and poor COVID-19 outcomes.
Authors
Additional authors on the study are Frederick Cudhea and Renata Micha at the Friedman School, and Junxiu Liu, a postdoctoral scholar at the Friedman School at the time of the study, now assistant professor at the Icahn School of Medicine at Mount Sinai.
Funding
This work was supported by two awards from the National Institutes of Health's National Heart, Lung, and Blood Institute (R01HL130735 and R01HL115189). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. See the study for conflicts of interest.
Citation
O'Hearn, M., Liu, J., Cudhea, F., Micha, R., & Mozaffarian, D. (2021). COVID-19 hospitalizations attributable to cardiometabolic conditions in the U.S.: A comparative risk assessment analysis. Journal of the American Heart Association.