Research paves the way to early diagnosis of diabetic neuropathy
In the study, a group led by Professor Paulo Barbosa de Freitas Júnior measured grip force in diabetic patients while they were holding and handling objects. The results were compared with data for healthy subjects and patients with other neurological diseases, such as multiple sclerosis, Parkinson’s, and carpal tunnel syndrome (pain, numbness and tingling in the hand and arm caused by a pinched nerve in the wrist).
Freitas and his group tested volunteers to measure the grip force exerted by diabetics with and without a diagnosis of neuropathy, as well as healthy subjects, and developed a methodology that can be used to produce equipment for use in clinical practice. In future, the innovation should help physicians diagnose the disorder quickly and easily not long after the onset of initial symptoms of neuropathy in diabetics.
The analysis focused on grip force used to hold and manipulate objects, and on relative safety margin, i.e. grip force normalized by the coefficient of friction between skin in contact with the object and surface of the manipulated material. The central nervous system “calculates” the amount of force needed to hold an object, learning to do so better over time. “Every object has a contact surface with which our fingers create friction when we hold it. The smoother the surface, the more grip force needed to hold it. If it’s rough, we can use less grip force thanks to friction,” Freitas explained.
Considering grip force and safety margin, people with neurological disorders such as multiple sclerosis and Parkinson’s tend to use more force to grip objects than healthy people. The force needed to manipulate an object is moderately greater than the minimum force needed to hold it in the desired position. “In the case of people with neurological alterations, our hypothesis is that they grip objects more strongly as a conservative strategy,” Freitas said. “The nervous system detects a neurological deficiency and sends a command for the hand to use more force as it grips the objects. This process is entirely unconscious, of course.”
The test results showed that healthy volunteers used between 100% and 120% of the minimum force required to hold an object, whereas the force used by participants with neurological alterations was two and a half times to three times greater.
Freitas and his team then investigated the performance of diabetics, who typically suffer from neuropathy as the disease worsens. “There was no prior research on diabetics involving the type of experiment we used in our study,” he said.
The hypothesis was that diabetics would grip objects more tightly, as is the case with people who suffer from carpal tunnel syndrome, multiple sclerosis and Parkinson’s. “However, what we found was the opposite: diabetics used half as much force to hold an object as controls in the simplest task, which was the static test, in which the subject merely has to hold an object without manipulating it,” Freitas said.
An article published in the journal Human Movement Science reports the main findings of the study, which was funded by FAPESP via a Regular Research Grant and a scientific initiation scholarship.
Calculating grip force
Three types of test were conducted with 36 volunteers, including 24 diabetics divided into two groups: 12 who had developed neuropathy, and 12 who had neither been diagnosed with neuropathy nor displayed clinical signs of the disorder. The other 12 participants were healthy and formed the control group. Before testing began, the researchers measured each participant’s skin sensitivity, since the sense of touch is a key factor in conveying to the central nervous system the information required by the brain to calculate the force needed to hold and manipulate objects.
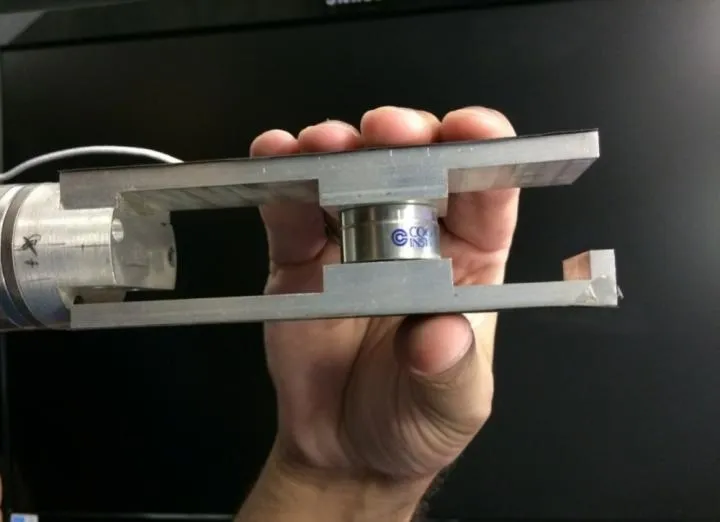
Volunteers were each asked to perform three tasks using the same type of object instrumented to measure force. In the static holding test, they had to hold the object with their dominant hand as if they were holding a glass of water. A beep sounded after ten seconds, and they were to unclasp their fingers slowly so as to release the object, while a researcher measured the friction between the fingers and the object. The second task consisted of picking up an object from a table, lifting it about 5 cm, holding it for 10 seconds, and putting it back on the table. In the third task, termed oscillation, the volunteers had to grasp the object, hold it in front of their navel, and move it about 20 cm up and down for 15 seconds.
In the second and third tasks, the results for diabetics and diabetics with neuropathy were similar to those for controls. The surprise came in the simplest task of all, which was static holding, as diabetics and diabetics with neuropathy used half the force applied by the controls.
The explanation is not exactly a loss of sensitivity in the fingers of diabetics, the researchers explained, but deficient tactile information sent from their fingertips to the central nervous system. There is not enough information of high quality for the brain to make the requisite calculations and the hand to use the right amount of force. “In addition, there are studies showing that certain areas of the spinal cord and cortex that receive and process this sensory information are smaller in diabetics than in healthy people,” Freitas said.
The study suggests diabetes does not only affect the periphery of the body, causing loss of sensitivity in the toes and fingers, for example, but also affects the central nervous system. “This happens early in diabetes. People tend to think these complications happen only after a certain age or when a person has had diabetes for some time, but actually patients have the problem before neuropathy is diagnosed,” Freitas said.
Novel device for rapid early diagnosis
Scientists do not fully understand what causes neuropathy in diabetics. One hypothesis has to do with neuron death or loss of function due to alterations in blood vessels and metabolism. “Because of metabolic alterations, blood doesn’t reach the nerve ends in the soles, palms, toes and fingers, leading to the death of neurons in these peripheral regions,” Freitas surmised. As the disease progresses, neurons in other regions closer to the torso, knees and so on, also suffer damage and may die.
Given this lack of knowledge, prevention is the best option, and the study discussed here will help in this regard, according to Freitas. “Our research provides a foundation on which a simple device could be developed for use in the doctor’s office with rapid results,” he said. Grip and load force can serve as behavioral biomarkers to detect neurological alterations even before the patient manifests clear symptoms of neuropathy. “The idea is to have a device that enables physicians to measure force in a straightforward test and see if the patient shows signs of incipient neurological alterations.”
Neuropathy is currently diagnosed by means of a painful invasive examination using a technique called electroneuromyography, in which an electric current is passed through small electrodes in the shape of needles inserted into the patient’s muscles and the reaction time is measured to assess nerve conduction velocity. Freitas proposes a procedure that can be used during a regular visit to the doctor. The patient would hold an object instrumented to measure grip force. “After 10 to 15 seconds of this test, the physician would have the result: the object was held with this or that level of force, and the value measured is below or above the level considered safe to the act of holding the object. It could evidence neurological alterations arising from diabetes,” he said.
The next steps envisaged by Freitas include developing the instrumented object for use in such testing, which could be simpler than the one used in research. To do so, he needs to determine the best combination between the object’s weight and surface smoothness or roughness, so as to evidence the difference between diabetics and nondiabetics. “We need various combinations of smoothness and roughness, as well as lighter and heavier weights, in order to measure the differences between the combinations, and choose the best for use in future tests,” he said. He is pursuing partnerships with hospitals and companies interested in participating in the development of a solution, as well as volunteers for forthcoming studies. He can be contacted at Paulo.deFreitas@cruzeirodosul.edu.br or defreitaspb@gmail.com.
INFORMATION:
About São Paulo Research Foundation (FAPESP)
The São Paulo Research Foundation (FAPESP) is a public institution with the mission of supporting scientific research in all fields of knowledge by awarding scholarships, fellowships and grants to investigators linked with higher education and research institutions in the State of São Paulo, Brazil. FAPESP is aware that the very best research can only be done by working with the best researchers internationally. Therefore, it has established partnerships with funding agencies, higher education, private companies, and research organizations in other countries known for the quality of their research and has been encouraging scientists funded by its grants to further develop their international collaboration. You can learn more about FAPESP at http://www.fapesp.br/en and visit FAPESP news agency at http://www.agencia.fapesp.br/en to keep updated with the latest scientific breakthroughs FAPESP helps achieve through its many programs, awards and research centers. You may also subscribe to FAPESP news agency at http://agencia.fapesp.br/subscribe.