Can a blood test track ovarian cancer through its structural DNA chaos?
Oncoscience / MD Anderson Cancer Center / UC San Diego
High-grade serous ovarian cancer is defined by structural violence at the chromosomal level. The genomes of these tumors are shattered and rearranged, with large-scale deletions, inversions, and translocations that distinguish them from most other cancers. What if those very rearrangements — the structural variants that make HGSOC so aggressive — could serve as personalized beacons in a patient's blood?
That is the question a team led by Jian Li at MD Anderson Cancer Center and corresponding author R. Tyler Hillman at UC San Diego set out to answer. Their approach, published in Oncoscience, flips the usual liquid biopsy strategy. Instead of hunting for single-nucleotide mutations in circulating tumor DNA, they targeted the unique chromosomal breakpoints created when a tumor's genome rearranges itself.
Designing a probe for each patient's tumor
The workflow starts with whole-genome sequencing of tumor biopsies — not from one site, but from multiple locations within each patient's cancer. From that sequencing data, the team identified patient-specific structural variant breakpoints: the exact positions where chromosomal segments were cut and rejoined during tumor evolution.
They then designed custom primer and probe sets that span those breakpoints. Think of it as creating a molecular fingerprint unique to each person's cancer. These assays were first validated on synthetic cell-free DNA derived from ovarian cancer cell lines to confirm they could reliably detect the targeted breakpoints at low concentrations.
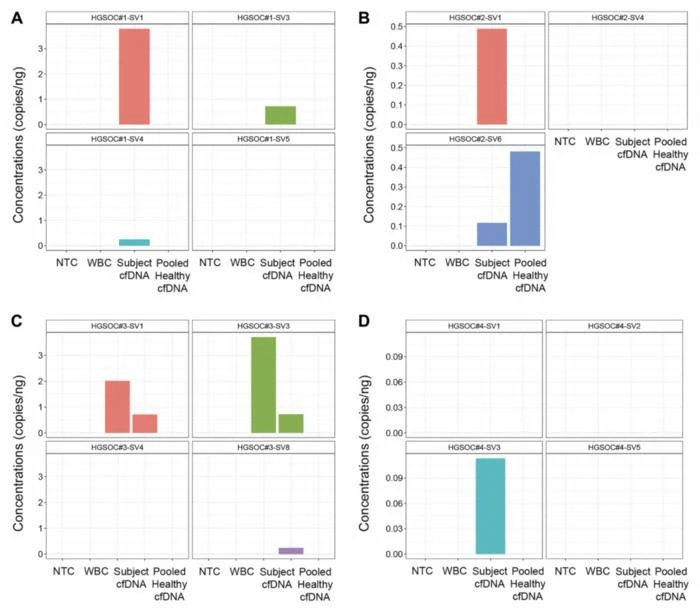
Once optimized, the assays were applied to pre-treatment plasma samples from four HGSOC patients. From the whole-genome sequencing data, the team designed and validated 29 tumor-informed breakpoint assays. Of 15 assays selected for testing on cell-free DNA, nine produced measurable signals in the corresponding blood samples.
Why structural variants instead of point mutations?
Most existing liquid biopsy platforms track single-nucleotide variants — individual letter changes in the DNA code. These work well for cancers driven by recurrent point mutations, like certain lung or colorectal cancers. But HGSOC is a different beast. Its defining molecular feature is not a handful of hotspot mutations but widespread chromosomal rearrangement.
Structural variants, by their nature, create entirely novel DNA sequences at the breakpoint junctions — sequences that exist nowhere in the normal human genome. That specificity is a significant advantage. A positive signal is almost certainly tumor-derived, reducing false positives.
The team also found that digital droplet PCR (ddPCR) outperformed standard real-time PCR for this application. ddPCR partitions each sample into thousands of individual droplets, counting positive signals one by one rather than relying on amplification curves. The result is greater sensitivity at the vanishingly low DNA concentrations typical of early-stage or post-treatment blood samples.
Four patients and a proof of concept
The study is explicitly a pilot. Four patients. Pre-treatment samples only. No longitudinal tracking through chemotherapy cycles, no comparison with existing commercial liquid biopsy platforms. The researchers are transparent about these constraints.
The approach also requires whole-genome sequencing of tumor tissue and custom assay design for each patient, which adds cost and turnaround time compared to off-the-shelf ctDNA panels. For a monitoring tool to be clinically useful, those practical barriers matter as much as the underlying science.
Still, the feasibility data are clear. Nine of 15 validated assays detected tumor-derived structural variants in plasma. That detection rate, in a cancer type where liquid biopsy options remain limited, is worth pursuing.
Where the trail leads next
The authors outline a concrete path forward: prospective testing in larger patient cohorts, streamlined bioinformatics pipelines to shorten the time from biopsy to assay, longitudinal blood sampling through treatment to test whether structural variant levels correlate with response and relapse, and head-to-head comparison with mutation-based liquid biopsy platforms.
If those studies confirm what this pilot suggests, tumor-informed structural variant monitoring could complement existing tools — particularly for cancers where chromosomal rearrangement, not point mutation, drives the disease. HGSOC is the obvious first application, but the principle could extend to other cancers dominated by structural genomic changes.
So does tracking chromosomal chaos in the blood actually work for ovarian cancer? In four patients, with custom-built probes and a sensitive detection method, the answer appears to be yes. Whether that translates into a clinical tool that changes how doctors monitor treatment response remains an open question — one that will require considerably more patients and longer follow-up to answer.